Tibialis Posterior dysfunction(Pes planus),Treatment
Posterior tibial tendon dysfunction (PTTD) is a painful and disabling condition of the foot and lower extremity that most commonly affects women over the age of 60.
The main pathology of PTTD is thought to begin with some form of internal damage to the posterior tibial (PT) tendon. The tendon may develop a partial tear, elongate, degenerate or may even completely rupture.

Weakness of the posterior tibial muscle due to the tear of tendon will tend to increase the pes planus deformity. over the period of time it is due to loss of the important supination effects of the muscle.
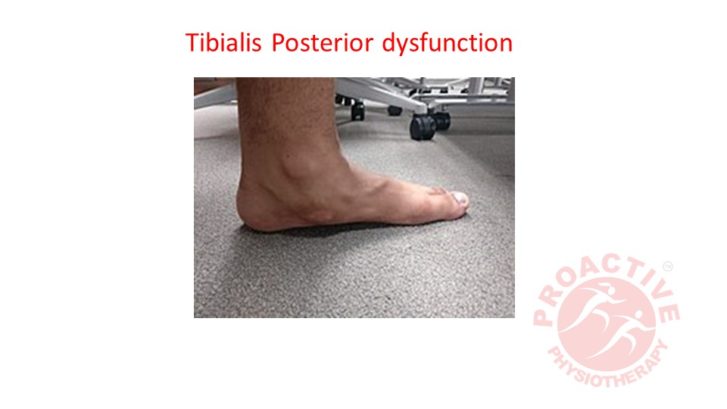
Patients with PTTD very commonly indicated with a “flatfoot” or “pronated foot” before the pain and disability has began. According to author all PTTD patients have demonstrate a medially deviated Sub talar joint axis (STJ). The tibialis posterior muscle has mechanically disadvantaged due to changes in STJ axis . hence, it can’t generate normal magnitudes of internal STJ supination moment even before the symptoms of PTTD begin (see photo below).
The medial deviated STJ axis not only requires increased internal STJ supination moments from the tibialis posterior muscles but also causes a decreased supination moment arm for the tendon. see illustration
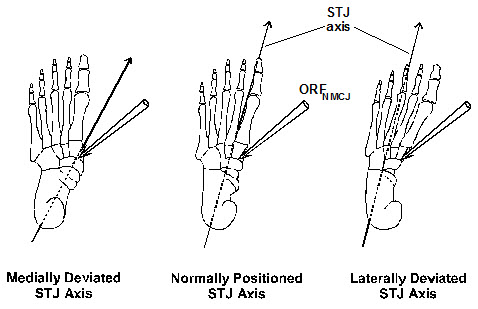
above).The mechanical result of this pre-existing medially deviated STJ axis in the individuals who ultimately develop PTTD is increased PT tendon tension forces, which greatly increases the tension stress within the PT tendon.
Tibialis posterior tendon damage causes weakness and/or pain in the muscle which results in decreased STJ supination moment and leads to increased external STJ pronation moments acting from ground reaction force (GRF). The increased STJ pronation moments eventually lead to increased tension stress on the spring ligament complex which may result in its partial or complete rupture, along with other plantar ligaments which help support the longitudinal arch of the foot. Tearing of the spring ligament will specifically cause further longitudinal arch flattening and also forefoot abduction on the rearfoot.
In order to stop the progression of flatfoot deformity that occurs in PTTD, the excessive external STJ pronation moments from GRF caused by the abnormally medially deviated STJ axis must be addressed with some form of mechanical foot therapy. Custom foot orthoses offer the simplest, most effective and most reliable method to treat PTTD by increasing the external STJ supination moments by shifting the ground reaction force which is more medially on the plantar foot.
Management:
Tibialis posterior dysfunction include a 3/16” to 4/16” polypropylene shell, a 2-6 mm medial heel skive, a 16-20 mm deep heel cup, a 2-4 mm heel contact point thickness and a minimal medial expansion plaster thickness and 1-5 degree inverted balancing position of the cast. The medial heel skive, when combined with the increased medial arch height of the inverted balancing position and minimal medial expansion plaster, work synergistically together to increase the STJ supination moment.

It is also quite important, in the earliest stages of treating the patient with PTTD, to make certain the patient is also placed into a shoe with a stable sole and relatively rigid construction. Alternatively, in more advanced cases of PTTD, a high top boot of some form in order to help brace the ankle and offer some resistance to STJ pronation by the bracing effect of the boot superior to the STJ axis. In addition, commonly use icing therapy for the PTTD treatment to reduce tendon edema and pain and use PT muscle strengthening exercises (invertors strengthening, toe curling) once the initial inflammation of the PT tendon starts to subside with treatment.
Referance:
- The medial heel skive technique: improving pronation control in foot orthoses. Kirby KA JAPMA, 82: 177-188, 1992).
- Subtalar joint axis location and rotational equilibrium theory of foot function. Kirby KA JAPMA, 91:465-488, 2001).
- Foot and Lower Extremity Biomechanics III: Kirby KA Precision Intricast Newsletters, 2002-2008. Precision Intricast, Inc., Payson, AZ, 2009, pp. 43-44
- Image coutsey google


Leave a Reply
Want to join the discussion?Feel free to contribute!