
Inter and Intrarater reliability of Hip muscles assessment
Clinically we are expected to assess all aspects of a patient’s musculoskeletal condition. However, it is challenging for us in the clinic to use valid and reliable measures to test the strength, so what are the clinical reliable tests are available to test hip muscle strength?
Let’s start with functional tests, crossly er al, all determined a single leg ) squat was sufficiently reliable in diagnosing those with hip muscle weakness. They devide the single leg squat performance in three category,of good, fair or poor.
They have not found difference in external rotation between ‘good’ and ‘poor’ groups. Moreover, there is no hip extension strength measures were taken. There is significantly less hip abduction strength with moderate or poor control . In addition , there is reduced in knee flexion and hip adduction range (quadriceps and ITB/tensor fascia latae shortening) . Again hip extension measures were not taken and no difference in external rotation was found.

Crossley et al (2009): Examples of Single Leg Squat. A) good performance; B) poor overall and trunk performance; C) poor pelvis and hip performance; D) poor hip and knee performance.
In both these studies, sitting as well as in prone hip external rotation was tested with the knees strapped together, and the force exerted against the tibia. The clamshell is also a hip external rotation movement, but it is more clinically relevant.
Selkowitz (2013) showed the clamshell has double the gluteus maximus torque compared to gluteus medius, with gluteus maximus being a primary extensor and eternal rotator of the hip.
Athletes with anterior knee pain, who typically display []poor Single leg Squat technique, show deficits in hip abductor, extensor and external rotator strength .The assessment of hip extension strength would be enlightening for us . This clearly indicates we need to assess all muscles around the hip, not just the abductors. (Prins & van der Wurff et al 2009)

Now Moving from functional assessment into specific muscle testing, various positions are required to assess hip muscle strength.
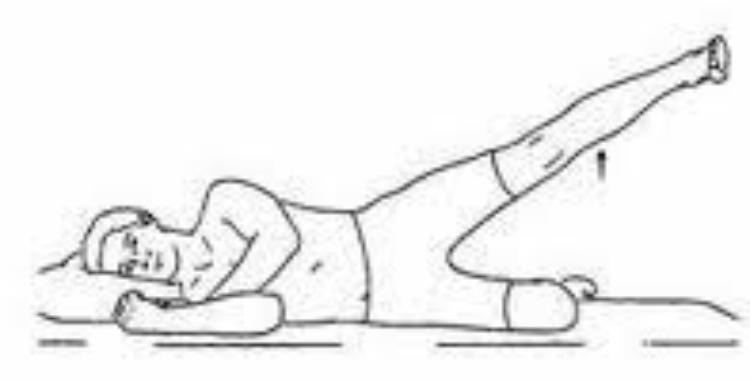
widler et al (2009) states in their study that Sidelying abduction is described as the most valid assessment for hip abduction strength, compared to supine and standing. (Perry, Weiss et al ,2004)describe in their study that using dynamometer Prone hip extension and supine hip extension (from 30° hip flexion, pushing against manual resistance towards the bed) are both shown to be valid and reliable in assessing hip extension.
There is strong reliability in assessing hip adductors in supine with resistance placed against the knees, pushing into abduction (Malliaras, Hogan, Nawrocki, Crossley, & Schache, 2009). The authors showed moderate intra-rater and inter-rater reliability when assessing internal and external rotation. The patient is in supine position with the foot hanging over the bed, with the hip in neutral and knee in 90° flexion, then exerting force against the medial or lateral malleolus.
When assessing hip strength, a perceived exertion or repetitions to fatigue may be more clinically relevant. If the patient displays Grade 5/5 hip extension strength but had poor control on left single leg squat, it may be more appropriate to measure prone hip extension repetitions to fatigue. This prevents a ceiling effect and allows a more specific reassessment at risk for future sessions.
Things to remember :
• Functional assessment –
[restrict] a poor single leg squat or step down highlights poor hip control, most likely hip abduction, extension and external rotation weakness.
• Specific testing –
• hip flexion – supine, resistance at 45° hip flexion
• extension – prone, knee 90° flexed
• abduction – sidelying (see picture above)
• adduction – supine, adduct against resistance
• internal/external rotation – hip neutral with knee 90° flexed over edge of bed (see picture above)
• Use number of repetitions to fatigue, perceived exertion if patient achieves Grade 5/5 on manual muscle testing.
This study identified that the clinical assessment of performance on the single-leg squat is a reliable tool that may be used to identify people with hip muscle dysfunction.
References:
- Malliaras, P., Hogan, A., Nawrocki, A., Crossley, K., & Schache, A. (2009). Hip flexibility and strength measures: reliability and association with athletic groin pain. British journal of sports medicine, 43(10), 739-744.
- Park, K.-M., Cynn, H.-S., & Choung, S.-D. (2013). Musculoskeletal predictors of movement quality for the forward step-down test in asymptomatic women. The Journal of orthopaedic and sports physical therapy, 43(7), 504-510.
- Perry, J., Weiss, W. B., Burnfield, J. M., & Gronley, J. K. (2004). The supine hip extensor manual muscle test: a reliability and validity study. Archives of physical medicine and rehabilitation, 85(8), 1345-1350.
- Selkowitz, D. M., Beneck, G. J., & Powers, C. M. (2013). Which exercises target the gluteal muscles while minimizing activation of the tensor fascia lata? Electromyographic assessment using fine-wire electrodes. The Journal of orthopaedic and sports physical therapy, 43(2), 54-64.
- Widler, K. S., Glatthorn, J. F., Bizzini, M., Impellizzeri, F. M., Munzinger, U., Leunig, M., & Maffiuletti, N. A. (2009). Assessment of hip abductor muscle strength. A validity and reliability study. The Journal of bone and joint surgery. American volume, 91(11), 2666-2672.
- Crossley, K. M., Zhang, W.-J., Schache, A. G., Bryant, A., & Cowan, S. M. (2011). Performance on the single-leg squat task indicates hip abductor muscle function. The American journal of sports medicine, 39(4), 866-873.
- Prins, M. R., & van der Wurff, P. (2009). Females with patellofemoral pain syndrome have weak hip muscles: a systematic review. The Australian journal of physiotherapy, 55(1), 9-15.
- Google image pic courtsey
[/restrict]

