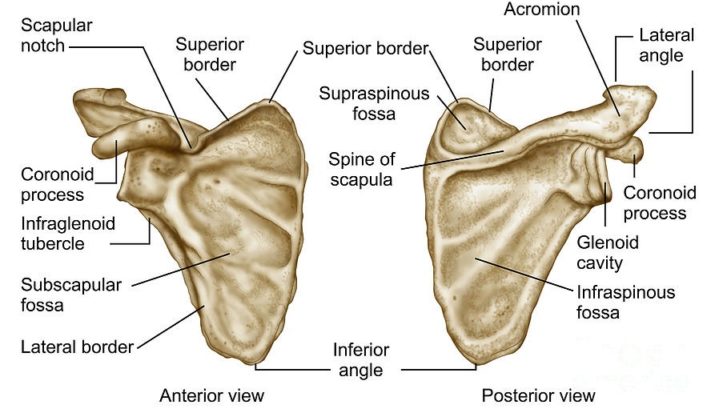
Clinical assessment of scapula
Upper limb is designed in such a way that there is ample amount of mobility which is required for manipulative activities that are a part of daily functional activities. In recent days there is increased interest on the role of scapula, its related pathologies and how entire upper extremity function is dependent on the controlled movement of scapula.
For a full, efficient as well as atleast functional range of motion of entire upper limb, scapula plays many roles in facilitating optimal shoulder function by glenohumeral integration, motion on thoracic wall and as a part of scapula-humeral rhythm. With good proximal control there is good distal mobility. Any alterations in the activity of scapula hamper the control over all upper limb activities leading to pain, impingement and other clinical syndromes which gradually causes disability.
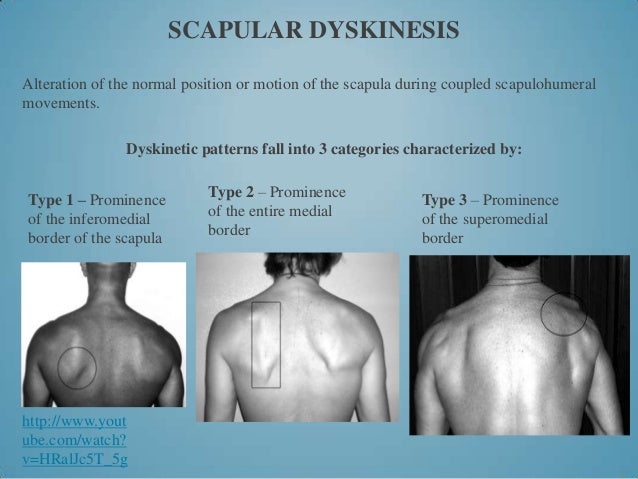
Observable alterations in the position of the scapula & the pattern of scapular motion in relation to thoracic cage are called scapular dyskinesis. It causes many clinical dysfunction of the shoulder leading to disabilities.
Causes of Scapular Dyskinesia:
- Bony injuries or abnormalities- Types of acromion process or postural alteration

- .Alteration of muscle function- upper cross syndrome, inhibited muscle- serratus anterior, lower fibres of trapezius, rhomboids, deep neck flexors, force couples.

- Contracture & other flexibility problems- pectoralis minor & major, joint capsule, upper fibres of trapezius, levator scapula
- Nerve injury/ proprioceptive dysfunction- long thoracic nerve, spinal accessory nerve
Classification of Scapular Dyskinesia:
 (Slideshare.net)
(Slideshare.net)
- Type I – Abnormal rotation around transverse axis: commonly found secondary after rotator cuff dysfunction- inferior angle becomes prominent
- Type II – Abnormal rotation around vertical axis: commonly seen in patients with glenohumeral joint instability- medial border becomes prominent
- Type III – Abnormal superior translation of entire scapula: commonly seen in rotator cuff dysfunction and deltoid-rotator cuff force imbalances- superior border becomes prominent
- Type IV- both scapula are symmetrical at rest & during motion; they rotate symmetrically upward with inferior angles rotating laterally away from midline. This indicates scapular control muscles are not stabilizing the scapula.
Types of Winging:
- Static winging- winging happens at rest, usually caused by structural deformity of scapula, ribs, clavicle or spine.
- Dynamic winging- winging happens with shoulder motion. It can be cause of trapezius weakness or serratus anterior weakness. In case of trapezius weakness, scapula depresses and moves move laterally with inferior angle rotated laterally. In case of serratus anterior weakness, scapula elevates amd move medially with inferior angle rotated medially.
One more clinical syndrome exists which is coined as S.I.C.K scapula–
[restrict]
S- Scapular mal-position
I- Inferior angle prominent
C- Coracoid pain
K- Dyskinesia
Clinical assessment of scapula includes evaluating posture, motion, muscular activation and control and corrective maneuvers. Steps for assessment
- History taking
- Thoracic and cervical posture – trigger points and flexibility
- Check for the shoulder posture- trigger points and flexibility
- Shoulder strength – especially supraspinatus, infraspinatus, and subscapularis, Serratus anterior, lower trapezius
- Shoulder ROM @ 0 and 90 degrees – GIRD
- Scapula position @ rest
- Scapula position during active abduction and flexion – especially watch descending phase
- Scapulothoracic bursitis
Few important tests include Lennie test, Lateral scapular slide test, Scapular assistance test, scapular isometric pinch test, wall push test, Labral tests, impingement tests, tendinitis tests, etc.
References
- Kibler B, McMullen J. “Scapular dyskinesis and its relation to shoulder pain”. J Am Acad Orthop Surg. 2003;11:142-151.
- Magee DJ. “Shoulder. Orthopaedic Physical Assessment.” 5th Philadelphia: WB Saunders. 2012; 231-360.
[/restrict]
. To read more register on our website


Leave a Reply
Want to join the discussion?Feel free to contribute!