PECTORALIS MINOR- THE NEGLECTED MUSCLE

Human body is designed in such an intricate manner that upper limbs are for manipulative activities and lower limbs are for mobility. When each of the body segments is aligned properly it gives a pleasant appearance as well as a disorder free body. While poor posture and muscular imbalance often results into pain and loss of function.
Physiotherapy musculoskeletal assessment format consists of many points in observation, palpation and examination which are extremely important for proper diagnosis, treatment planning and knowing the prognosis. However, many a times while assessing shoulder and cervical region; one of the important muscle- Pectoralis Minor is often neglected. A shortened pectoralis minor muscle commonly contributes to muscular imbalance and pain in shoulder and cervical region.
Poor upper body posture is many a times referred to as a ‘forward head posture’, ‘slouched posture’, ‘poking chin posture’, or ’rounded shoulder posture’ and is considered to be a potential etiological factor in the pathogenesis and perpetuation of many clinical syndromes like Thoracic outlet syndrome, Scapular downward rotation syndrome, Scapular winging & tilting syndrome, shoulder impingement syndrome and also upper cross syndrome involving the neck and shoulder.1, 2

The pectoralis minor attaches at the coracoid process of the scapula and at the third, fourth, and fifth ribs near their sternocostal junctions. A short pectoralis minor muscle increases the muscles passive tension with arm elevation resulting in restriction of normal scapular movements such as external rotation, upward rotation and posterior tipping and this in turn will affect glenohumeral and cervical motion.1, 3
Few Clinical tests have been recommended to test for shortening of this muscle.
AT Distance: 1, 4, 5
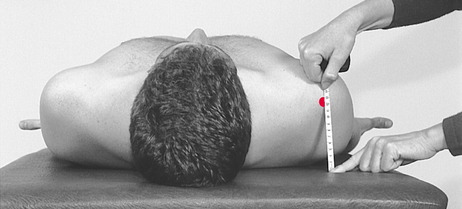
The patient in supine lying, arms by side or resting on abdomen and instructed to relax. With the help of rigid standard plastic transparent right angle, measure the linear distance in millimeters between the posterior border of the acromion and the table. Take care not to exert any downward pressure into the table and place the base on the treatment table and the vertical side adjacent to the lateral aspect of the acromion. A distance greater than 2.54 cm (1 inch) suggests short pectoralis minor.
Pectoralis Minor Length Index (PMI): 1, 4, 5, 6
The PMI is calculated by dividing the resting muscle length measurement by the subject height and multiplying by 100.The resting muscle length is measured between the caudal edge of the 4th rib to the inferomedial aspect of the coracoid process with a measuring tape or sliding caliper. PMI is suggested to reflect a shortened pectoralis minor when 7.65 or lower.
Referances :
- Jain S, Shukla Y. “To find the intra-rater reliability & concurrent validity of two methods of measuring Pectoralis Minor tightness in Periarthritic Shoulder patients.” Indian Journal Of Physical Therapy 2013;1(2):34-38
- Lewis J.S., Valentine R.E. “The Pectoralis minor length test: a study of the intra-rater reliability & diagnostic accuracy in subjects with & without shoulder symptoms.” BMC Musculoskeletal Disorders. 2007; 8:64.
- Borstad J.D. “Resting position variables at the shoulder: Evidence to support a posture-impairment association.” Journal of the American Physical Therapy Association. 2006; 86(4):549-557.
- Borstad J.D. “Measurement of Pectoralis Minor Muscle Length: Validation and Clinical Application.” Journal of Orthopaedic and Sports Physical Therapy. 2008; 38(4):169-174.
- Struyf F., Nijs J., Mottram S., Roussel N., Ann M J Cools, Meeusen R. “Clinical assessment of the scapula: a review of the literature.” Br J Sports Med 2012;0:1–8.
- Muraki T, Aoki M., Izu.mi T, Fujii M., Hidaka E., Miyamoto H. “Lengthening of the pectoralis minor muscle during passive shoulder motions & stretching techniques: a cadaveric biomechanical study.” Phys Ther. 2009; 89(4).
- Pic : Netter`s Anatomy


Leave a Reply
Want to join the discussion?Feel free to contribute!