There are many tests reported in the literature, commonly including:
- McMurray’s
- Apley’s compression
- Joint line tenderness
- Thessaly’s
- End range flexion/extension overpressure
This conclusion must be taken with caution since frequent methodological design flaws exist within the included studies, most studies suffered from various biases, and between-study heterogeneity makes pooled data unreliable.”
We don’t even do the Apley’s compression test. Never saw a value, like the Thessaly Test. Nice in theory but just not good enough when tried in a clinical practice.
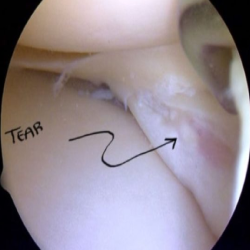
Even need to Diagnose Meniscus Tears?
We must accurately diagnose and explain to the patient that many people have meniscal tears in their knee when they have trauma . The recent literature builds a strong case for a very good recovery without surgery. That’s right, surgery is often not needed for many people diagnosed with a meniscus tear.
This paper really created waves when it was released in 2013. They stated that “outcomes after arthroscopic partial meniscectomy were no better than those after a surgical procedure.”
Don’t get me wrong, surgery may be needed, especially for the people sustaining an acute meniscus tear. But that may only be a small portion of the people presenting to us in the clinic.
In these people, We reduce the inflammation and restore ROM , strength and see how they do. Maybe a 6 week PT course is all they need, you never know.
The research does not support using these tests to diagnose and may add to the fear avoidance a patient may exhibit after such a diagnosis. This systematic review and meta-analysis in the British Medical Journal stated:
“The results of this systematic review indicate that the accuracy of McMurray’s, Apley’s, JLT and Thessaly to diagnose meniscal tears remains poor.
What meniscus tests do do?
[restrict]we believe in clinical examination which is very important to help guide the treatment plan.
The exam NEEDS to match the clinical history.
According to patient history and it’s problem, you should decide the test.So,here is the test :
- Joint line palpation
- End range flexion/extension pain/locking
- McMurray’s (but often not very valuable)
- Apply’s test , Thessaly test
We would say joint line palpation and end range of motion are my 2 most valuable tests. We do the McMurray’s test to see if it can add to the clinical findings.
You all have question in your mind that why We didn’t even mention the Thessaly test. why we want to put our patient in a weight-bearing position, which is already painful knee.
Never mind the research telling us that the test is not very valid which goes completely against early research that said it was a valid test.
we may need to combine this test with others to help improve our accuracy in examination as stated in this paper .in this paper “Five positive findings on composite examination yielded a positive predictive value of 92.3%. Positive predictive values remained greater than 75% with composite scores of at least 3 in the absence of ACL and DJD pathologies.”
Keep in mind that the particular side of the meniscus tear may influence the ability to detect a pathology. Era net al said in his paper 2009, Lateral meniscal tears may be easier to distinguish than medial meniscal tears if we’re talking about joint line tenderness alone.
Take home message:
- Proper clinical examination
- Understand what tests are best to deploy.
- sticking with our in-depth history,
- Joint line tenderness and end range flexion and extension test are useful
I’m pretty sure it has done us well over the years…and the research seems to match my thoughts too.
Read our previous post on meniscus rehabilitation
[/restrict]
To Read More Register Now or Log in

