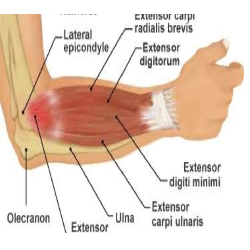
Lateral epicondylgia is commonly known as a tennis elbow is described as a tendinopathy of a common extensor origin. It commonly occurs in athletes, especially tennis players. It also occurs in the people who do repetitive heavy work with hands.
Most treatment approaches include, strengthening and stretching of wrist extensors and forearm supinator, iontophoresis, splinting & bracing, NSAIDs, local cortisone injections.
A recent study reported a recurrence rate of 29% to 38% in individuals receiving conservative treatment.1 In the only study with a 2-year follow-up after physical therapy intervention, more than half the patients reported ongoing pain and function loss secondary to the return of LE symptoms.
Most of us do not include scapular muscle while treating lateral epicondylgia. This has always been suggested by clinical therapists. There are also some researches which have supported this hypothesis.
Lucado et al3 recently reported diminished lower trapezius (LT) muscle strength in a group of female tennis players with LE compared to a matched group of asymptomatic female tennis players.
Alizadehkhaiyat et al4 dentified weaker rotator cuff musculature in patients with lateral epicondylalgia compared to that of a control group, but did not address scapular musculature strength.
Joseph M day and colleagues conducted a cross sectional study on scapular Muscle Performance in Individuals with Lateral Epicondylalgia. They took 28 patients with symptomatic LE and 28 controls matched by age and sex were recruited to participate in the study. Strength of the middle trapezius (MT), lower trapezius (LT), and serratus anterior (SA) was measured with a handheld dynamometer. A scapular isometric muscle endurance task was performed in prone. Changes in muscle thickness of the SA and LT were measured with ultrasound imaging. Analysis-of-variance models were used to determine within- and between-group differences.
They concluded that when compared to a matched comparison group, there were impairments of scapular musculature strength and endurance in patients with LE, suggesting that the scapular musculature should be assessed and potentially treated in this population.
Clinical importance
So while treating LE with conventional treatment we must include lower trapezius, middle trapezius and serratus anterior.
Exercise programme:
Trap
Patient can hold for10 seconds at the end range and repeat it 10 times
Lower Trap
Serratus Anterior
Push up plus –https://youtu.be/5C1M9ms20jI.
And/ or
https://m.facebook.com/story.php?story_fbid=1128855643805342&id=1110549392302634&_rdr.
References
1. Coombes BK, Bisset L, Brooks P, Khan A, Vicenzino B. Effect of corticosteroid injection, physiotherapy, or both on clinical outcomes in patients with unilateral lateral epicondylalgia: a randomized controlled trial. JAMA. 2013;309:461-469.
http://dx.doi.org/10.1001/jama.2013.129
2. Nilsson P, Baigi A, Swärd L, Möller M, Månsson J. Lateral epicondylalgia: a structured programme better than corticosteroids and NSAID. Scand J Occup Ther. 2012;19:404-410. http:// dx.doi.org/10.3109/11038128.2011.62098.
3. Lucado AM, Kolber MJ, Cheng MS, Echternach JL, Sr. Upper extremity strength characteristics in female recreational tennis players with and without lateral epicondylalgia. J Orthop Sports Phys Ther. 2012;42:1025-1031. http://dx.doi. org/10.2519/jospt.2012.4095
4. Alizadehkhaiyat O, Fisher AC, Kemp GJ, Vishwanathan K, Frostick SP. Upper limb muscle imbalance in tennis elbow: a functional and electromyographic assessment. J Orthop Res. 2007;25:1651-1657. http://dx.doi.org/10.1002/ jor.20458.
5. Scapular Muscle Performance in Individuals With Lateral Epicondylalgia. JOSEPH M. DAY, PT, PhD, OCS, CIMT • HEATHER BUSH, PhD ARTHUR J. NITZ, PT, PhD, ECS, OCS• TIM L. UHL, PT, ATC, PhD, FNATA

