Posterior Oblique Subsystem (POS)
Before reading this article click on introduction to core subsystem
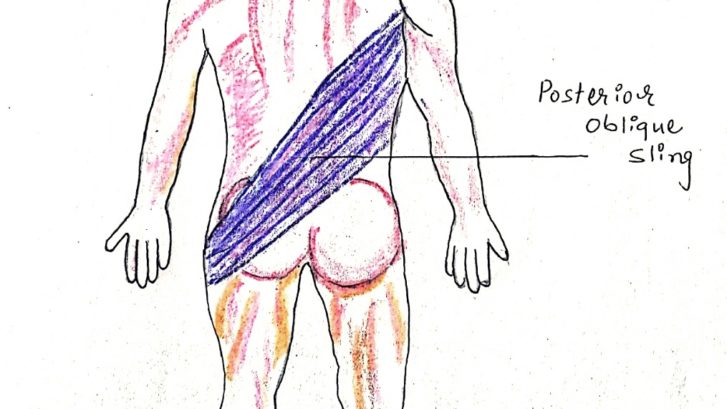
Structures are involved :
- Latissimus dorsi,
- Thoracolumbar fascia,
- Gluteus maximus
- Superior portion or gluteus medius.
Function (Brief):
IT stabilize the posterior kinetic chain Which including lumbar spine and sacroiliac joint. It transfers the force between us upper extremity and lower extremities eventually, integrated pulling movement of a body.
- Eccentric deceleration of total body
- Transference of force between lower and upper extremities
- Maintaining alignment of the lumbosacral joints
- Maintaining femoral alignment during legs with pull
Functional Arthrokinematics:
This subsystem is an important stabilizer of the posterior kinetic chain. The fiber arrangement in such a way i.e subsystem indicate a special role in sacroiliac joint (SIJ) arthrokinematics, and lumbo-sacral function.
The fibers of each side run perpendicular which crossing from the gluteus maximus and associated it’s respective fascia which traversing the SIJ, through the nearly continuous thoracolumbar fascia, across the lumbar spine, to the latissimus dorsi and associated fascia on the opposite side.
During the swing phase of gait cycle, the eccentric control of leg and contralateral arm pulls the thoracolumbar fascia tight. Concurrently, the contralateral Posterior oblique subsystem concentrically contracts throughout the gait cycle , which in turn pulls the contralateral side of the thoracolumbar fascia.
Optimal function of POS is to stabilize posture.
Motor Behavior:
The POS could be underactive termed in upper body dysfunction, Lumbo Pelvic hip complex dysfunction, sacroiliac joint dysfunction , and lower leg dysfunction. Commonly, the under-activity of the POS is paired with a synergistic dominance of the deep longitudinal subsystem (DLS – publish soon).
How to find POS underactive?
AOS may be dominance seen in upper body dysfunction and who present lower leg dysfunction that results in excessive forward lean during the overhead squat assessment. It indicates POS is
[restrict]
underactive. By doing squat assessment clinician will find out which subsystem is dominance and underactive. Many of times we find the patient is not able to do full squat though he has full ROM (without any pathology involvement). It may indicate POS is underactive.
Exercise Selection:
If overhead squat movement assessment presents with signs of POS under-activity, consider the following changes to your exercise programming.
Core: Use the bridge progression as part of your routine to strengthen the gluteus maximus. If the AOS is also dominant it may be beneficial to discard crunches, planks and chops exercise. Start with clam she’ll exercise progress to hip side abduction.
Above all exercise, pelvic must be a neutral position. If proper recruitment occurs it’s easy to break up overactive subsystem.


The summaries above are intended for a quick reference in practice and do not illustrate all possible scenarios.
Reference:
1. Dr. Mike Clark & Scott Lucette, “NASM Essentials of Corrective Exercise Training” 2011 Lippincott Williams & Wilkins
2. Donald A. Neumann, “Kinesiology of the Musculoskeletal System: Foundations of Rehabilitation – 2nd Edition” 2012 Mosby, Inc.
3. Carolyn Richardson, Paul Hodges, Julie Hides. Therapeutic Exercise for Lumbo Pelvic Stabilization – A Motor Control Approach for the Treatment and Prevention of Low Back Pain: 2nd Edition Elsevier Limited, 2004
image coursey : http://paspapt.com/low-back-pain
https://www.runnersworld.com/injury-treatment
[/restrict]
To Read More Register Now


Leave a Reply
Want to join the discussion?Feel free to contribute!