
Gluteus Maximus Activation: Optimal position
Kan, S., Jeon, H., Kwon, O., Cynn, H., Choi, B. (2013). Activation of the gluteus maximus and hamstring muscles during prone hip extension with knee flexion in three hip abduction positions. Manual Therapy 18, 303-307

Why this study relevant for us ?:
The gluteus maximus is a commonly under-active muscle within the predictive models of Sacroiliac Joint Dysfunction (SIJD). This particular article focuses on the gluteus maximus as the prime mover of hip extension. The hamstrings and adductor magnus are synergistic muscles contributing to hip extension, with the biceps femoris likely contributing most to hip extension force production after the gluteus maximus. Synergists tend to become overactive when prime movers are inhibited. Therefore, an exercise that allows for optimal alignment of the gluteus maximus while limiting over activity in the hamstrings.
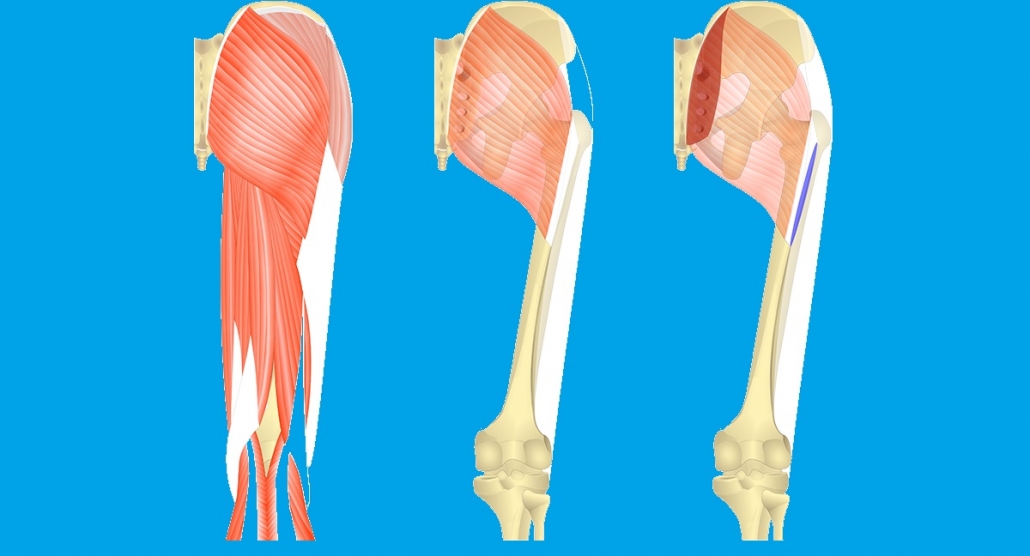
Note the oblique fiber alignment and attachment sites of the gluteus maximus. Hip abduction during extension provides a direct line of pull which increases gluteus maximus activation.
Review:
The overall methodology for this study was strong despite the small sample size. Researchers implemented clear processes and procedures to improve the validity of the data obtained. Hip extension was performed with a bent knee to place the hamstrings into a position of active insufficiency therefore it is limiting excessive synergistic assistance. Further, For standardized assessment researchers create a wooden boards guided the appropriate amount of hip abduction required. There should not excessive knee flexion or hip rotation during hip extension. Any deviations were visually note by examiner relative to the wooden structure. If minimal deviations were observed than data for those repetitions was discarded. Subjects practiced the task for 5 minutes to eliminate errors of unfamiliarity.
Researchers placed the gluteal EMG electrode at an oblique angle to match the muscle fiber orientation, to ensure the validity and integrity of surface EMG data. Measurements were determined by averaging three trials in each plane of hip abduction with 30 seconds rest in between each trial. Subjects rested two minutes between each trials. The degree of abduction used in a particular trial was determined randomly via a computer program and was referenced using a line drawn from the subject’s ASIS through the center of the subject’s patella. This study is not without limitations. Lumbar extension during hip extension did not consider but they were careful to minimize compensatory knee and hip movement patterns. It is unclear in this study that any subject achieved the desired end position (holding the patella 5cm above the table) using pure hip extension or any used compensatory lumbar extension.
In addition to that, researchers evaluated shortened muscles and the presence of pain but did not assess other movement impairments which could indicate poor hip biomechanics. The EMG electrode place between the greater trochanter and the S2 vertebra. It may allow for potential interference from the piriformis and deep rotators of the hip. These muscles are commonly overactive; however, such interference may be unlikely given their depth and the placement of the electrode on the center of the gluteus maximus muscle belly. For a standard set up, the authors chose to use only one electrode for gluteus maximus and one electrode for the hamstring muscles but the study would have benefited from the use of two separate EMG machines with two electrodes per muscle. Last, it would be interesting to evaluate gluteus maximus and hamstring EMG activity with hip extension with the knee extended and compare those findings in this study.
Clinical commentary:
This research is important because the relationship between a prime mover and synergist muscles during a particular movement pattern. Specifically, it documented gluteus maximus and hamstring (activity during prone hip extension with a bent knee at different degrees of hip abduction (0 degrees, 15 degrees, 30 degrees). The authors findings including the orientation of muscles fibers alignment of gluteus maximus muscles. Gluteus maximus has fusiform shape muscle fibers which run parallel to the long axis of the muscle and generate direct tension when the muscle contracts. When consider pelvic girdle to the attachment site the gluteus maximus fibers run obliquely on the femur and iliotibial band, and therefore hip abduction may improve muscle recruitment through better fiber alignment.
When the efficiency of a prime mover can be enhanced,(eg. the gluteus maximus with 15 degrees (or more) of hip abduction) synergistic muscles will likely be less capable of dominating activity.
In 0 degrees of hip abduction, the hamstrings fired first with greater intensity because the gluteus maximus fibers did not have optimal alignment for motor unit recruitment. However, in 15 and 30 degrees of abduction, the gluteus maximus fired sooner than the hamstrings and with greater intensity. This study provide evidence of an optimal line of pull to better activate an inhibited and/or weak gluteus maximus while limiting compensatory synergistic actions of the hamstrings.
How does this affect practice?
Prone hip extension with a bent knee is a commonly used during manual testing and strengthening of gluteus maximus. Performing hip abduction while extending the hip with a bent knee offers better recruitment of the gluteus maximus and limits synergistic assistance of the hamstrings.
Additionally, once the gluteus maximus is activated, the nervous system will minimize output to its synergists to create pure hip extension without compensation. In addition to increasing gluteus maximus activation for rehabilitation or strengthening purposes, when looking to isolate the gluteus maximus hip abduction should be greater than 15 degrees. It may also provide a more optimal manual muscle test position.The degree of abduction used for consistency between assessments that should keep in mind.
Image courtesy: google

