Sub acromial impingement and scapular downward rotation syndrome.
Ideal scapular alignment is described as the vertebral border parallel to the spine and positioned 3 in. from the midline of the thorax (Sobush et al., 1996). The scapula is normally positioned between the spinous process of the second and seventh thoracic vertebrae and rotated 30 anterior to the frontal plane (Kendall et al., 2005; Magee, 1997; Sahrmann, 2002; Hoppenfeld, 1976). Alteration in normal scapular alignment affects muscle balance, sacpulo-humeral rhythm during arm movements, neck-shoulder pain, stability of glenohumeral joint (Azevedo et al., 2008; Kibler and Sciascia, 2010; Reinold et al., 2009).
The alignment of scapula is important for optimal functioning of the shoulder joint (Kibler and Sciascia, 2010). Additionally, when the inferior border of the scapula is more medial than the superior border, the scapula is considered to be in SDR; the shoulder is lower and slopes downward at the acromial end (Caldwell et al., 2007). Changes in alignment of the scapula and clavicle can potentially influence the biomechanics of the shoulder region by altering tension at the cervicoscapular muscle (increased upper trapezius muscle length, and levator scapula stiffness), which may lead to insufficient scapular upward rotation, instability of the glenohumeral joint, thoracic outlet syndrome during arm elevation, and prolonged compressive loading of the cervical spine (Sahrmann, 2002; Caldwell et al., 2007; Szeto et al., 2002). The clavicle is the sole bony structure connecting the trunk to the shoulder girdle via the sternoclavicular joint medially and the acromioclavicular joint laterally (Ljunggren, 1979).
During arm elevation in the scapular plane, individuals with subacromial impingement exhibit decreased scapular upward rotation, increased scapular internal rotation(winging)(weak SA) and anterior tilt (weak lower trapezius), and decreased subacromial space width, compared to those without subacromial impingement. Altered scapular muscle activity is commonly associated with impingement syndrome.
Study shows that scapular upward rotation exercises improved the alignment of scapula and clavical and also improved the scapular upward rotator muscle strength.
Scapular upward rotation exrcises (SURE);
SURE instruction was provided to the subjects by asking them to stand with their back against the wall, with wall contact from head to buttock, and feet shoulder-width apart.
In the starting position, the radial border of the forearms and lateral side of the humerus were in contact with the wall, and the shoulder was abducted 90 with the elbow flexed 90. The subjects were instructed to slide their arms up the wall. The sliding movement ended when the shoulder reached 180 of abduction. For ensuring of scapular upward rotation during SURE (non-resistive SURE or resistive SURE), subjects were asked to contact the tip of the shoulder with earlobe in the end point of SURE.
Lower trapezius exercise :
Patient in standing position, arm by side, now ask patient to take the shoulder backward & downward ( Retraction and Depression . This will activate lower trapezius.
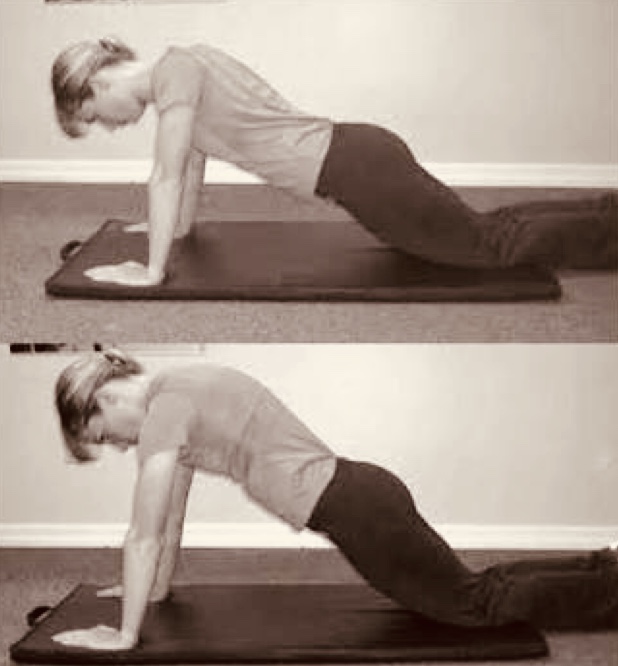
Serratus anterior exercise: