Shoulder Impingment : How do you approach
we previously written about impingement and contribution of scapula now in this article you will understand how to differentiate impingement type. Shoulder impingment ios usually common terminology in shoulder pain that we oftnly use in our daily practice.
We usually label any pain originated around shoulder we directly say its ” Shoulder impingement”
The use of such a broad term as a diagnosis purpose which is not helpful to determine the treatment process. There is no any fix protocol for shoulder impingement that you can address for all the patients.
That is the reason why conclusions are difficult to be drawn from meta-analysis and systematic reviews. A thorough examination can be used to determine the best treatment plan. Every patient is different for us and its diagnosis. We will require variations for their shoulder rehabilitation.
We do specific test for shoulder impingment involves provocation test. Those test are great but people are confuse for their shoulder pain, they can`t figure our where exactly pain is locating.
Shoulder Impingement: Assessment and Treatment
I make treatment process more simple and address only certain things to differentiate shoulder impingement. Below are the points that needs to be consider
1. The location of shoulder pain
2. The structures involved
3. The underlying cause of shoulder impingement
we previously written about impingement and contribution of scapula now in this article you will understand how to differentiate impingement type. Shoulder impingment ios usually common terminology in shoulder pain that we oftnly use in our daily practice.
We usually label any pain originated around shoulder we directly say its ” Shoulder impingement”
The use of such a broad term as a diagnosis purpose which is not helpful to determine the treatment process. There is no any fix protocol for shoulder impingement that you can address for all the patients.
That is the reason why conclusions are difficult to be drawn from meta-analysis and systematic reviews. A thorough examination can be used to determine the best treatment plan. Every patient is different for us and its diagnosis. We will require variations for their shoulder rehabilitation.
We do specific test for shoulder impingment involves provocation test.
Each of these can significantly vary the treatment approach. If you approach each patient with above three things in mind, you are going to do better job developing an effective treatment plan, versus hopefull treatement plan. If you apply the same treatment protocol for every shoulder patient than you may get only 20-30% result or you make them worst and simply waste of time.
Let’s drilling through shoulder joint……….
Location of Shoulder Impingement
The first things that needs to consider is location of impingement.This impingement reference to side of rotator cuff. Is it located either outside or undersurface of rotator cuff.
These are two type either:
1. Bursal sided shoulder impingement – this is your traditional subacromial impingement
2. Articular sided shoulder impingement – this is called internal impingement
Bursal Sided Shoulder Impingement

See the above photo of a shoulder MRI above. The bursal side is the outside of the rotator cuff, shown with the blue arrow. This may be your your “standard” subacromial impingement that most people refer to when simply stating “shoulder impingement.”
This is called subacromial impingement because of the location of impingement occurs between the rotator cuff and the undersurface of the acromion, hence the term “subacromial.” This is also called the bursal side of the rotator cuff because there is a bursa located between the rotator cuff and the acromion, which acts as a shock absorber.
2. Articular Side:
The yellow arrow shows the undersurface, or articular surface, of the rotator cuff. This Impingement side is often termed “internal impingement” because the impingement occurs on the inside of the rotator cuff.
The internal impingement often involves the supraspinatus and infraspinatus rotator cuff muscles. The undersurface of these two muscles impinges against the glenoid joint rim. The two types of impingement are completely different and occur for different reasons.
We move our arm daily that actually “impinge” every thing. It’s becomes abnormal, excessive, or too frequent that shoulder pain and pathology occurs.This is the reason we straight away say “impingement”. Its true, some impingement is normal but excessive impingement may cause pain and lead to pathology.
when the structures involved in impingement, try to differentiate between subacromial and coracoacromial arch impingement. These can happen in combination or isolation and involve the supraspinatus muscle.There Is mild modifications for coracoacromial and subcoracoid impingement, which we will discuss below.
Bursal sided impingement:
* Subacromial impingement – Involves the supraspinatus and acromion
* Coracoacromial impingement – Involves the supraspinatus and coracoacromial arch
* Subcoracoid impingement – Involves the subscapularis and coracoid
Articular Sided:
* Internal impingement – Involves the supraspinatus and infraspinatus and glenoid rim. They have different location and different injury mechanism. we now have differentiated and know the cause but still don’t know “why” the person has impingement.
Cause of Shoulder Impingement
There are two main classifications of causes that I refer to as “primary” or “secondary” shoulder impingement.
Primary Shoulder Impingement
Primary impingement means that the impingement is the main problem with the person.
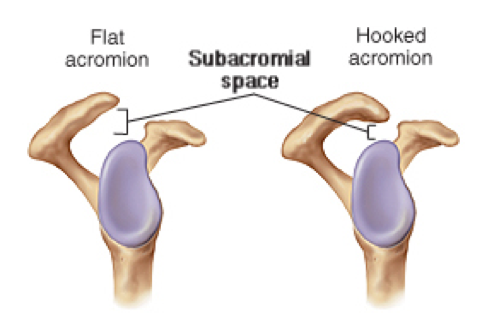
Eg: someone that has impingement due a hooked tip of the acromion like this in the picture below. Many acromions are flat or curved, but some have a hook or even a spur attached to the tip.
From our clinical experience of shoulder joint improves, it appears that the larger a bone spur, the more problem for rotator cuff to glide beneth acromion.This is referred to as primary impingement. Hence, There is no effect on mobility, strength, and dynamic stability as there is a primary cause of impingement which causing the symptoms.
Defiantly, we may improve the symptoms and often times are successful with rehabilitation, but sometimes we lose the match against shoulder rehabilitation. It’s not because a certain treatment “isn’t effective for shoulder impingement.” It’s because there is a primary reason why impingement is occurring that we can’t change.
Secondary Shoulder Impingement
Secondary impingement means that something else is causing impingement. It may be activities, posture, lack of dynamic stability, or muscle imbalances. There are causing the humeral head to shift in its center of rotation and cause impingement which is due to rotator cuff dysfunction. The rotator cuff and larger muscle groups, like the deltoid, work together to move your arm in space. Both muscles groups need to work together.

If rotator cuff does not work properly, It may lose its ability to keep the humeral head centered. In this condition, The deltoid will overpower the cuff and cause the humeral head to migrate superiorly, thus impinging the cuff between the humeral head and the acromion. This is just a simple example. It’s not just weakness of the rotator cuff, it’s also imbalanced strength ratios and improper firing time of dynamic stabilization.(subscapularis) There are other reasons for secondary impingement which include mobility restrictions and poor dynamic stability of the shoulder, scapula, and even thoracic spine. All of these areas need to work together to produce optimal shoulder function.
Lets understand from clinical case, In the picture below, the person does not have full overhead mobility. If we did with this person was treat the location of the pain in his anterior shoulder, our success will be limited. when he will return to the gym and start the process all over if we don’t restore this mobility restriction.
Differentiating Between the types of Shoulder Impingement
The two most popular special tests for shoulder impingement are the Neer and the Hawkins test.


In the Neer test, the examiner stabilizes the scapula while passively elevating the shoulder, in effect impinging the humeral head into the acromion.
In the Hawkins test, the examiner elevates the arm to 90 degrees of abduction and forces the shoulder into internal rotation, impinging the cuff under the subacromial arch.
As I mentioned earlier, these special tests are provocative in nature, meaning that we are looking for reproduction of pain.
Both of them will cause the structures to impinge in all of us, but they shouldn’t produce pain. But if the area is sensitive and irritable, they will cause pain.
You can alter these tests slightly to see if they elicit different symptoms that would be more indicative to the coracoacromial arch or subcoracoid types of subacromial impingement. because these structures are more anterior, we can alter the tests to better assess this area.
The Neer test can be performed in the sagittal plane, and the Hawkins test can be modified and performed in a more horizontally adducted position. Both of these positions will impinge more anteriorly.
Many patients with subacromial impingement may be symptomatic with all of the above tests, but you may be able to detect the location of subacromial impingement (acromial versus coracoacromial arch) by watching for subtle changes in symptoms with the above four tests.
Just like we’ve talked about with the studies looking at the treatment effectiveness in people with shoulder impingement, most studies published vaguely look at how accurate a test may be at detecting “impingement.” Hopefully, if you’ve gotten this far in the article, you see how flawed this approach is, as this is simply too broad.
How can we evaluate how “specific” a special test is for such a “non-specific” diagnosis?
This type of impingement is most commonly seen in overhead athletes, It is typically the result of hyperlaxity of the shoulder in the anterior direction. As the athlete comes into full external rotation ( tennis serve, volleyball serve) the humeral head slides anterior slightly causing the undersurface of the cuff to impingement on the inside against the posterior-superior glenoid rim and labrum.
The best special test for internal impingement is the same as an anterior apprehension test:
The examiner externally rotates the arm at 90 degrees abduction and watches for symptoms. Unlike the shoulder instability patient, someone with internal impingement will not feel apprehension or anterior symptoms. Rather, they will have a very specific point of tenderness in the posterosuperior aspect of the shoulder (below left). When the examiner relocates the shoulder by giving a slight posterior glide of the humeral head, the posterosuperior pain diminishes (below right).

Treating Different Types of Shoulder Impingement
As we hope you can treat shoulder impingement. you should differentiate between subacromial, coracoacromial, subcoracoid, and internal impingement. Treatment is similar between these types of impingement. There is a bunch of overlap.However, there are some differences:
- Subacromial impingement: you should be very cautious with overhead activities that produce discomfort.
- The more anterior-based coracoacromial arch and subcoracoid impingement: elevation in more of a sagittal plane and horizontal adduction movements that produce discomfort.
- Internal impingement: Excessive external rotation at 90 degrees abduction (like the throwing position) that produce discomfort.
You should not work through discomfort or a “pinch” with impingement.A “pinch” is impingement of a sensitive structure!
Treating Primary Versus Secondary Shoulder Impingement
If you are dealing with secondary impingement, you can treat the person’s symptoms. we want to reduce discomfort and inflammation. This is going to allow us to do more in the long term. However, this should not be the primary focus if you want long term success.
We should look global at the patient. Their posture, muscle imbalances, and movement patterns all come into play. You should have a systemized way of assessing movement and building programs to optimize and enhance their function. A good discussion of the activities that are causing their symptoms may also shed some light on why they are having shoulder pain.

As you ion the picture above , if you don’t have full mobility and try to force the shoulder through this motion restriction you are going to likely cause some irritation. We usually spend a great deal of time discussing what range of motion the person should be working . Essentially, we try to develop a 0-100* and a 100*-full ROM depending on when they have symptoms. It’s important to continue working within their 0*-100* and not simply say “take a few weeks off.” And slowly over time, our goal is to expand their Range of motion.
Treating Internal Impingement
The internal impingement is going to occur with any cuff weakness, fatigue, or loss of the ability to dynamically stabilize. The overhead athlete will show some hyperlaxity in of external rotation. Most overhead athletes have underlying laxity. They lose strength or have an excessive workload that causes fatigue and gradually the structures impingement more and become irritable. Treat the cuff weakness and its ability to dynamically stabilize to relieve the impingement.
How to approach to treat impingement?
The algoritham summarises a clinical reasoning algorithm the clinician may use in the treatment of scapular dyskinesis. There are Flexibility deficits which need to be addressed by stretching and mobilisation techniques.
In the therapist’s decision-making and clinical reasoning process, a thorough clinical examination should precede the choice of treatment goals and appropriate techniques and exercises.
In the early stage of scapular training, conscious muscle control of the scapular muscles may be necessary to improve proprioception and to normalise the scapular resting position. Following the scapular orientation exercises, scapular co-contraction. it may be exercised in basic positions, movements and exercises.
Specific exercise for control the scapula.


Inferior Glide:
The IG is an isometric exercise that emphasizes humeral head depression and scapular retraction the scapular muscles primarily targeted for this exercise were the SA and LT. Person will be in an upright sitting
position with the test arm abducted to 90° with fist clenched on a firm supportive surface. person will instruct to apply pressure with his or her fist in the direction of arm adduction and instructed to inferiorly
depress their scapula and hold this position for 5 seconds.
Low Row:
This is an exercise that emphasizes scapular external rotation and posterior tilt. The scapular muscle primarily targeted in this exercise were the SA and LT. Person stood in front of an immovable surface. Person placed their hand on the anterior edge of the surface with palm facing posteriorly. Instruction was given to extend their trunk and push their hand maximally against the surface in the direction of shoulder extension and instructed to retract and depress the scapula the isometric contraction was performed for 5 seconds.
Lawnmower
This exercise used the motion of hip/trunk extension, trunk rotation, and scapular retraction to activate the muscles to assist in positioning the scapula in retraction. These multijoint exercises use force-dependent integrated muscle activation patterns to coordinate the motions of connected joints and to produce efficient and stable distal joint positions
through the production of interactive moments. the exercise with their
trunk flexed and rotated to the contralateral side from the
instrumented arm with their hand at the level of their contralateral
patella. Person was instructed to rotate the trunk toward the instrumented arm and extend the hip and trunk to a vertical orientation while simultaneously placing their instrumented arm at waist level and retracting
their scapula so that they try to place an “elbow into their
back pocket” position.
Robbery exercise
It is a multijointed exercise that uses hip/trunk extension and bilateral arm motion to achieve scapular retraction. Person began in a standing position with the trunk flexed to approximately 40° to 50° with arms forward flexed and palms facing the thighs. While keeping the elbows close to the body, moved into trunk and arm extension and flexed the elbows so palms were facing up and away from the body while simultaneously pinching both scapulae toward his or her back pockets with a strong 5-second contraction.
Rotator cuff strengthening

These isotonic exercises can be coupled with a standing external rotation exercise with elastic tubing as well as the external rotation oscillation exercise, which uses 30-s sets and elastic resistance to provide a resistance bias to the posterior rotator cuff using an oscillating device. Other advantages of the use of a towel roll or pillow to place the shoulder in
approximately 20–30° of abduction are preventing decreased blood flow in the supraspinatus tendon and increasing the subacromial space

Exercises using 90° of glenohumeral joint abduction and the scapular plane serve to apply the specificity principle to middle-stage rehabilitation
and prepare the athletic patient for the positions used during a
return to both throwing . In addition to traditional external rotation exercise in the scapular plane elevated position, the use of both
oscillation and rhythmic stabilisation or perturbations applied
by the clinician can be used to add additional challenges to the
exercise and increase the number of repetitions applied in the
exercise session.

Plyometric exercises for the posterior rotator cuff in overhead athletes are also used in the later stages of rehabilitation in the 90/90 position.
References:
1] Kibler WB, Sciascia AD, Uhl TL, et al. Electromyographic analysis of specific exercises for scapular control in early phases of shoulder rehabilitation. Am J Sports Med 2008;36:1789–98.
2]Kamkar A, Irrgang JJ, Whitney SL. Nonoperative management of secondary shoulder impingement syndrome. J Orthop Sports Phys Ther 1993;17:212
3]Mottram SL. Dynamic stability of the scapula. Man Ther 1997;2:123–31.
4] Ludewig PM, Cook TM. Alterations in shoulder kinematics and associated
muscle activity in people with symptoms of shoulder impingement. Phys Ther 2000;80:276–91.
5]Roy JS, Moffet H, Hébert LJ, et al. Effect of motor control and strengthening exercises on shoulder function in persons with impingement syndrome: a singlesubject study design. Man Ther 2009;14:180–8.
Pic courtesy : Google


Leave a Reply
Want to join the discussion?Feel free to contribute!