
Understanding extension pattern back pain: an overuse injury (Members only)
Low back pain is common in the general population, with rates as high as 84 percent reported. Low back pain is less common in athletes, accounting for only about 6-10% of injuries, trailing the more common ankle, knee, and shoulder injuries. Because low back pain in athletes involves only minor pain and dysfunction, the majority of athletes continue to train and compete. However, some severe pathologies result in more severe pain and dysfunction. When there is back pain, perform a thorough exam and differential diagnosis to rule out:
• Herniated lumbar discs, with or without radicular pain and radiculopathy. Spondylolysis, followed by pars interarticularis defects and spondylolisthesis.
• Pain in the zygapophyseal (facet) joint.
• Fracture of the facet joint
• Kissing Spine, also known as Baastrup’s disease.
• Pain in the sacroiliac joint.
• Stenosis of the spine.
• Ankylosing spondylitis is an example of a genetic group.
Patterns of pain in extension
Extension pain patterns, first described by Shirley Sahrmann as part of her kinesiopathologic model of movement dysfunction, are a subset of the larger group of dysfunctions known as Movement System Impairment (MSI) classification and syndromes. The basic premise of the MSI classification is that repetitive direction-specific movements can cause microtrauma and tissue stress in passive and active elements such as ligaments and muscles, resulting in low back pain.
It is difficult to pinpoint the exact source of pain in these extension pain patterns. Facet joints, ligamentous tissue creep or stretch, nociceptive fibres in the intervertebral disc, or ischemia in the paraspinal muscles can all cause pain.
Pattern of active extension
Active extension movements cause pain by overloading the lumbar spine structures. These could be long-term extension forces or frequent moderate-load extension movements. Active paraspinal muscle contraction increases compressive forces on the lumbar facets. Athletes and sports with this type of back pain presentation include:
1. Runners who have hyperlordosis. The paraspinal extensors contract constantly in this posture to keep the pelvis anteriorly tilted. Prolonged extension and anterior pelvic tilt can cause muscle ischemia and pain on either side of the lumbar spine.
2. CrossFit athletes – Those who perform repetitive extension-based lifts, such as a deadlift ladder or Olympic weightlifting movements, generate high compressive forces on the facet joints when in extension. Because this type of activity is more intermittent, muscle-based pain is unlikely, and the clinician should look for pain in the facet joints.
Rowers who sit with excessive lordosis and maintain a lordosis during the pull phase of the stroke may experience joint or disc pain.
4. Cricket, swimming, and tennis – The fast bowl, butterfly stroke, and tennis serve all require rapid active extension movements that can cause pain in the facet joints, ligaments, and discs.
Low-level facet joint irritation is one source of pain in the active extension pain pattern. Three direct mechanisms(2) contribute to facet loading in the active extension pattern:
Compressive loading of the articular process against the vertebral laminae below. Muscle contraction that is active and increases compression.Spinal rotation that causes the articular processes to rub together.
Facet loading is therefore more common in sports involving compressive forces, such as CrossFit, and axial rotation, such as tennis. Early facet degeneration is common in adolescent tennis players, and 70% of elite teenage tennis players have at least one level of facet arthropathy.
Athletes with a swayback posture and a kyphotic thoracic spine may exhibit this pain pattern. When the athlete moves into extension positions, the lumbar spine is forced into passive extension to compensate for the thoracic area’s lack of extension. This pattern is common in sports requiring low-velocity extension, such as:
1. Dance and gymnastics – As part of their performance, athletes must hold certain extension poses.
2. Tennis and swimming – This occurs as a result of the athlete’s time spent with arms extended overhead.
3. Golf and cricket – Athletes and golfers spend a lot of time standing still.
These activities have a more static extension. As a result, the source of pain is less likely to be muscular and more likely to be caused by ligamentous tissue creep and facet joint irritation caused by the compressive forces produced by the sustained postures.
How to recognise facet joint syndrome?
In several critical ways, extension pain patterns differ from more severe pathologies such as facet-joint syndrome. Because of the large number of nociceptive free nerve endings that innervate the structures, the facet joints themselves are the source of pain in facet joint syndrome. The synovial membrane, the hyaline cartilage surface of the articular processes, the bone itself, or the fibrous joint capsule can all cause facet joint pain. Facet-joint syndrome is most likely accompanied by degenerative lumbar spine spondylosis caused by progressive disc deterioration and shrinkage. The gradual decrease in disc height causes the facet joints to become more opposed and initiates a slow process of degeneration. Facet-joint syndrome has the following characteristics:
1. This is more common in older athletes/patients.
2. A history of low back pain in the past. Athletes exhibit normal gait.
3. Excessive pain with lumbar extension.
4. There is no pain aggravated by the Valsalva manoeuvre.
5. Lack of muscle spasms.

Clinical features of extension pattern pain
• Intermittent localised low back pain exacerbated by specific movements into extension postures is one of the more obvious clinical features of the active and passive extension pain patterns.
• Pain is typically bilateral and described as a “band across the back.”
• Rest or assuming a flexion posture relieves pain almost immediately. with pain, the athlete is frequently able to continue training and competing.
• Postural alignment is typically characterised by increased anterior pelvic tilt and increased lumbar lordosis, or a swayback posture.
• There is noticeable tension in the lumbar extensors and quadratus lumborum. Tensor fascia lata muscles are tense.
• When treating an athlete with extension-based low back pain, the clinician may become confused when distinguishing between more serious bone-related injuries, such as a pars stress reaction or fracture.
• The important factor is how quickly the pain subsides after the activity is stopped. The pain in the extension pain pattern cohort will almost immediately subside once the athlete stops the activity or moves into the opposite flexion direction.
Management
Low-intensity extension pattern pain syndromes are best managed conservatively, without the need for invasive facet joint steroid injections. Using a kinetic-chain approach, manage athletes by:
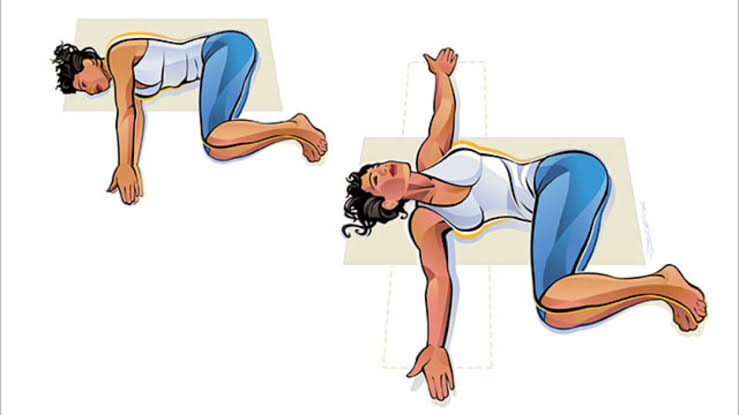
• Improving thoracic rotation to reduce lumbar rotation. Simple but effective mobility exercises include ‘bow and arrow’ and ‘thread the needle’ (see figures 1 and 2).
• Reducing hip internal and external rotator tightness. A decrease in hip rotation will result in an increase in lumbar rotation.
Improving the anterior hip muscles’ and anterior capsule’s hip-extension capacity.
• Reducing latissimus dorsi tightness, which can cause overhead athletes to compensate with lumbar extension. Increasing the strength of the abdominal and gluteal muscles, which control the posterior pelvic tilt.
☐ The following should be the focus of rehabilitation in the passive extension pain pattern cohort (who have the associated swayback posture):
• Lowering the thoracic kyphosis by lengthening the upper abdominals. Strengthening the thoracic extensors to help keep the thoracic spine in a neutral position.
• Increasing the strength of the deeper hip flexors, such as the iliacus, to move the hip out of extension and into a more neutral position.
Conclusion
Pattern of extension Low back pain is a type of mild low back pain experienced by athletes who participate in sports that require extension and anterior pelvic tilt. The most common cause of pain is benign facet joint irritation, ischemic muscle pain from prolonged contraction, ligament tissue creep, or low-level disc irritation. Managing this issue usually entails addressing any kinetic chain faults. These include limited hip extension, tight upper abdominals, limited trunk rotation, and abdominal/gluteal strengthening for athletes with excessive anterior tilt to raise awareness of the importance of maintaining a neutral spine posture during athletic movements.
Reference
- 1. Balagué F, Mannion AF, Pellisé F, Cedraschi C. Non-specific low back pain. Lancet. 2012 Feb 4;379(9814):482-91. doi: 10.1016/S0140-6736(11)60610-7. Epub 2011 Oct 6. PMID: 21982256.
- 2. Cohen SP, Raja SN. Pathogenesis, diagnosis, and treatment of lumbar zygapophysial (facet) joint pain. Anesthesiology. 2007 Mar;106(3):591-614. doi: 10.1097/00000542-200703000-00024. PMID: 17325518.
- 3. van Kleef M, Vanelderen P, Cohen SP, Lataster A, Van Zundert J, Mekhail N. 12. Pain originating from the lumbar facet joints. Pain Pract. 2010 Sep-Oct;10(5):459-69. doi: 10.1111/j.1533-2500.2010.00393.x. PMID: 20667027.
4. Allegri M, Montella S, Salici F et al. Mechanisms of low back pain: a guide for diagnosis and therapy [version 2; referees: approved] F1000Research 2016, 5(F1000 Faculty Rev):1530
")

