Shoulder instability can be fixed in 6 ways.

Due to the wide range of shoulder instability symptoms, it is crucial to comprehend a number of variables that will affect the rehabilitation process. This will enable us to tailor rehabilitation regimens for shoulder instability and speed up healing.
While creating my rehabilitation programs for nonoperative shoulder instability rehabilitation, I take into account six important elements. I’ll go through each in more depth.
Factor #1: Shoulder instability’s mechanism and recurrent nature
The cause and duration of the injury should be taken into account before beginning therapy for a patient with shoulder instability. There are two distinct categories of instability that include:
- Traumatic, acute instability
Atraumatic, ongoing instability
A sudden, traumatic incident or persistent, repeated instability may lead to pathological shoulder instability. Depending on how the injury occurred and how it happened, the rehabilitation program’s objective may change significantly.
The patient often comes with substantial tissue damage, discomfort, and anxiety after a violent subluxation or dislocation. In contrast to a patient who has subluxed their shoulder, the patient who has experienced a dislocation often displays greater discomfort as a result of muscular spasm. Also, a dislocation episode that occurs for the first time usually hurts more than one that occurs often.
The progression of rehabilitation will depend on the patient’s symptoms, with a focus on early controlled range of motion, a decrease in muscle guarding and spasms, and pain alleviation. Nonetheless, allowing the shoulder capsule to recover is the major objective.
Especially with first-time dislocations, the main traumatic dislocation is often treated conservatively with immobilization in a sling and early controlled passive range-of-motion (ROM) exercises.
The prevalence of repeated dislocation in patient groups between the ages of 21 and 30 years old varies from 17 to 96%, with a mean of 67%. Hence, the rehabilitation treatment for young athletes should go slowly. It should be mentioned that Hovelius has shown that the age of the patient determines the incidence of recurrent dislocations, which is unaffected by the time of post-injury immobilization. The majority of those who have numerous periods of instability are between the ages of 19 and 29. Hovelius also observed that patients in their 20s had a recurrence rate of 60% whereas individuals in their 30s and 40s had a recurrence rate of less than 20%. With an open physes, the recurrence rate in teenagers might reach 92%.
On the other hand, a patient with atraumatic instability often exhibits symptomatic symptoms and a history of recurrent injuries. The patient often complains chronic shoulder laxity or an inability to do certain activities rather than a single incident of instability.
Moreover, they often possess the capacity to move their shoulder in an excessive manner. many directions of instability too much cellular elasticity
Due to the patient’s particular characteristic of excessive capsular laxity and capsular redundancy, rehabilitation for this patient should concentrate on early proprioception training, dynamic stabilization drills, neuromuscular control, scapular muscle exercises, and muscle strengthening exercises to enhance dynamic stability.
Because to the lack of acute tissue injury, as well as the absence of muscle guarding and inflammation, chronic subluxations, such as those seen in the atraumatic, unstable shoulder, may benefit from more vigorous treatment. When ROM exercises are advanced, rotator cuff and periscapular strengthening exercises should be started. The joint capsule should not be too stretched by vigorous ROM exercises, it is advised.
Keep in mind that these people require stability more than movement.
Strength, proprioception, dynamic stability, and neuromuscular control are to be improved, particularly in the particular areas of motion or directions that give rise to complaints of instability.
Factor #2: Instability of the shoulders
The patient’s level of instability and how it affects their function make up the second element. There are many types of shoulder instability, such as mild subluxations and severe instability. The full separation of the articular surfaces with spontaneous reduction is referred to as shoulder subluxation.
In contrast, a dislocation completely separates the articular surfaces and must be moved or manually reduced in order to realign the joint. Trauma to the underlying capsular tissue will ensue from this. As a result, shoulder dislocations cause significantly more severe soft tissue damage to the glenohumeral joint.
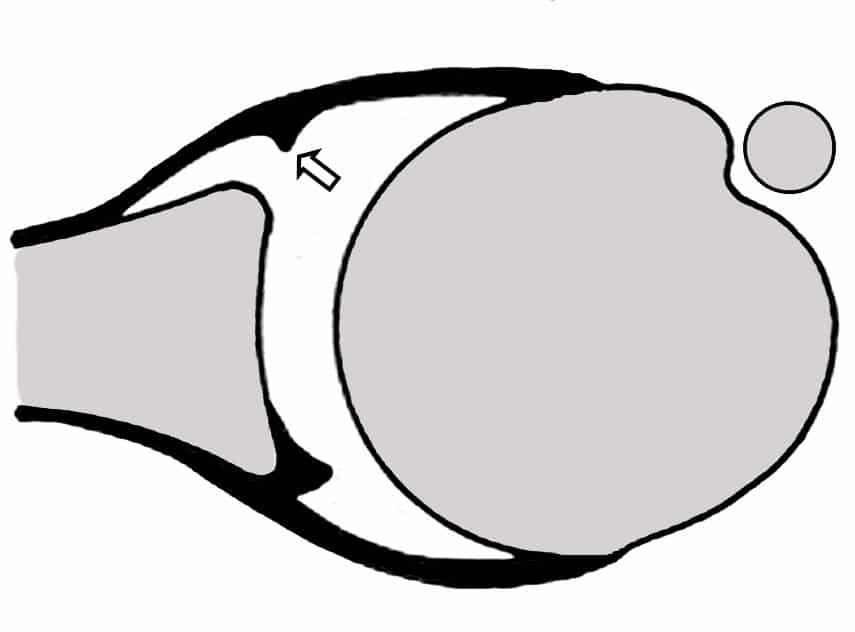
The anterior capsule may be avulsed from the glenoid in the case of an abrupt traumatic dislocation. The posterior capsule may be stretched in what is known as a Bankart lesion, causing the humeral head to dislocate. The “circular stability notion” has been used to describe this.
According to Speer, a Bankart lesion and soft tissue injuries on both sides of the glenohumeral joint capsule are required for a shoulder dislocation to take place.
Depending on the degree of instability and the duration of symptoms, the pace of progression will vary. A patient with minor subluxations and muscle guarding, for instance, could initially tolerate strengthening exercises and neuromuscular control drills better than a patient with a lot of muscular guarding.
This content is private. please select our membership plan to unlock the private content features.
And unlock the content.



