
Battle between two tribes
One of the major imbalances in treating individuals with lumbo-pelvic-hip pain and dysfunction involves the quadratus lumborum and gluteus medius. The quadratus lumborum is designed to contract to stabilize the ilia to allow proximal stabilization of the gluteus medius in order to control the femur with its distal attachment.
QL as having two divisions. The lower division arises from the medial portion of the iliac crest and adjacent iliolumbar ligament and inserts onto the transverse processes of the lumbar vertebrae,
The QL is primarily a coronal plane stabilizer causing lateral bending to the ipsilateral side when the foot is planted as well as posterior rotation of the lumbar spine on the weight bearing side. When acting unilaterally without the ipsilateral foot fixed on the ground, it can raise the ilia on the side of contraction. It is active during single limb support during stance phase of gait on the contralateral side (along with the external oblique) to elevate the ilium.
This is coupled with the ipsilateral anterior fibers of the gluteus medius and minimus pulling the iliac crest toward the stable femur. Sahrmann states “the QL is optimally situated to provide control of lateral flexion to the opposite side via its eccentric contraction to provide control of the return from lateral flexion via its concentric contraction. The muscle is also positioned to play a role in the rotation that occurs between the pelvis and spine during walking”.
Acting bilaterally, it extends the lumbar spine, deepening the lordosis and acting to limit anterior shear of the vertebral bodies.
Furthermore, it increased activation in response to increasing compression in static upright standing postures.
Assesment:
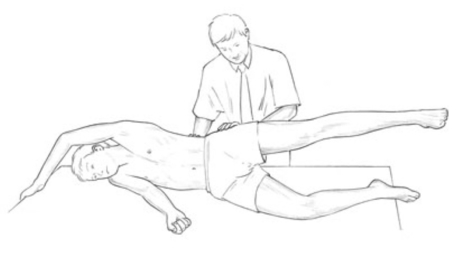
Palpation assessment for quadratus lumborum overactivity. The muscle is palpated, as is gluteus medius, during abduction of the leg. The correct firing sequence should be gluteus, followed at around 25° elevation by quadratus. If there is an immediate ‘grabbing’ action by quadratus it indicates overactivity, and therefore stress, so shortness can be assumed.
Clinical signs :
1) Sacroiliac joint dysfunction (upslip / superior translation) – this dysfunction creates a chronically tight QL which can lead to it becoming hypertonic as well which can lead to a hip hike during ambulation
2) Tight hip capsule / weak hip flexors – the body tries to maintain homeostasis of movement. If the hip is unable to flex, the central nervous system creates adaptation. To compensate, the hip (ilia) will hike to compensate for the lack of flexion.
3) Gluteus medius weakness – instability of lateral hip leads to excessive adduction during ambulation. In order to limit the amount of adduction, the hip will hike to decrease foot strike on the lateral foot. This leads to hypertrophy of the quadratus lumborum.
Treatment :
Quadratus lumborum MET method :
The patient lies supine with the feet crossed (the side to be treated crossed under the non-treated side leg) at the ankle. The patient is arranged in a light sidebend, away from the side to be treated, so that the pelvis is towards that side, and the feet and head away from that side (‘banana shaped’). As this sidebend is being achieved the affected quadratus can be palpated for bind so that the barrier is correctly identified.
MET treatment of quadratus lumborum utilising ‘banana’ position.
The patient’s heels are placed just off the side of the table, anchoring the lower extremities and pelvis. The patient places the arm of the side to be treated behind her neck as the practitioner, standing on the side opposite that to be treated, slides his cephalad hand under the patient’s shoulders to grasp the treated side axilla. The patient grasps the practitioner’s cephalad arm at the elbow, with the treated side hand, making the contact more secure.
The patient’s treated side elbow should, at this stage, be pointing superiorly. The practitioner’s caudad hand is placed firmly but carefully on the anterior superior iliac spine, on the side to be treated. The patient is instructed to very lightly sidebend towards the treated side. This should produce an isometric contraction in quadratus lumborum on the side to be treated.
After 7 seconds the patient is asked to relax completely, and then to sidebend towards the nontreated side, as the practitioner simultaneously transfers his bodyweight from the cephalad leg to the caudad leg and leans backwards slightly, in order to sidebend the patient. This effectively stretches quadratus lumborum. The stretch is held for 15–20 seconds, allowing a lengthening of shortened musculature in the region. Repeat as necessary.
Reference :

1) Muscle energy technique by Leon Chaitow


Leave a Reply
Want to join the discussion?Feel free to contribute!